Urinary tract infection
Disclaimer
These guidelines have been produced to guide clinical decision making for the medical, nursing and allied health staff of Perth Children’s Hospital. They are not strict protocols, and they do not replace the judgement of a senior clinician. Clinical common-sense should be applied at all times. These clinical guidelines should never be relied on as a substitute for proper assessment with respect to the particular circumstances of each case and the needs of each patient. Clinicians should also consider the local skill level available and their local area policies before following any guideline.
Read the full CAHS clinical disclaimer
|
Aim
To guide Emergency Department (ED) staff with the assessment and management of urinary tract infection in children.
Definition
Urinary tract infection (UTI) refers to a bacterial infection in the bladder (cystitis), or kidneys and ureters (pyelonephritis).
Background
- Urinary tract infections in childhood are common and can be potentially serious in the first few years of life
- The diagnosis of UTI should be considered in all febrile infants and young children, and in all infants with fever without focus.
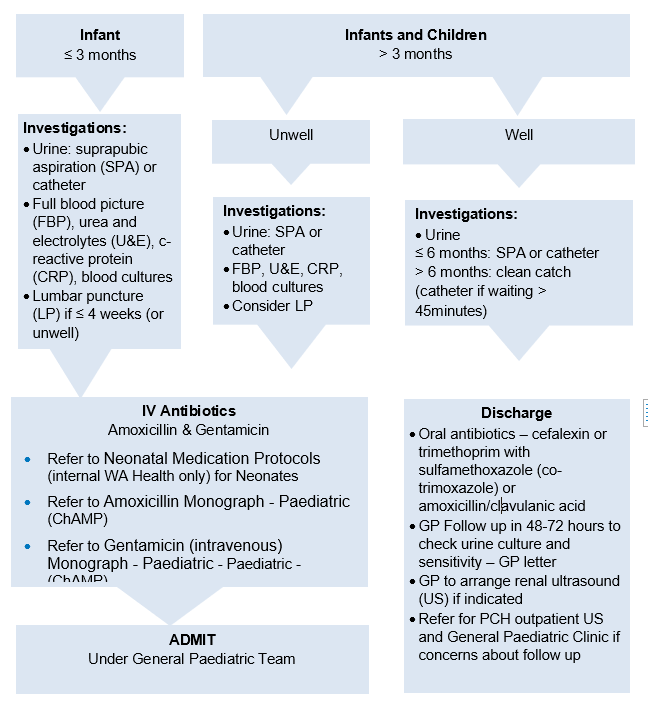
Urinary Tract Infection Management Flowchart
Assessment
- A reliable urine specimen is vital to confirm the diagnosis. Urine bags must not be used (high contamination rate).
- Suprapubic aspiration (SPA) is the gold standard in infants less than 6 months, however, in-out catheter specimens can be used. In infants and children over 6 months, in-out catheter specimens are the preferred choice if a clean catch specimen has not been achieved by 45 minutes.
- In febrile infants and children > 3 months who have a definite clear alternative clinical diagnosis, it is not necessary to check a urine collection in order to exclude a UTI.
History
- Fever may be present, particularly fever without apparent source
- Irritability
- Poor feeding
- Vomiting
- Jaundice (in neonates)
- In older children symptoms can include dysuria, urinary frequency, and urinary incontinence.
Investigations
- Urinalysis (dipstick) is not accurate in infants under 12 months - so cannot be used to exclude a UTI. The only urinalysis results reliably predictive of a UTI are the leukocyte esterase and nitrites.
- Urine should be sent to the laboratory for microscopy and culture.
- Send urgently in infants less than 6 weeks of age in whom a UTI is suspected
- After hours a microbiology technician will need to be called in after discussing with the on call microbiologist
- A reliable urine specimen is vital to confirm the diagnosis SPA, catheter, clean catch or mid-stream urine (MSU) in older children
- Urine cultures may be negative if there is previous antibiotic treatment
- Children who are systemically unwell and all infants less than 3 months should have blood tests including:
- Full Blood Count (FBC)
- Blood cultures
- CRP
- Urea, electrolytes and creatinine (UEC)
- Lumbar punctures should be done in neonates and children less than 6 weeks.
Investigations for age group
- FBC, CRP, UEC, blood culture
- Urine: SPA or catheter
- Lumbar puncture:
- ≤ 4 weeks: all children
- > 4 weeks: if unwell
|
Unwell
- FBC, CRP, UEC, blood cultures
- Urine
- ≤ 6 months: SPA or catheter
- > 6 months: clean catch or catheter if waiting > 45 minutes
- Consider lumbar puncture
Well
- Urine:
- ≤ 6 months: SPA or catheter
- > 6 months: clean catch or catheter if waiting > 45 minutes
|
Management
Management for age group
For more specific antibiotic information, refer to Urinary Tract Infection - Paediatric Empiric Guidelines (ChAMP).
Medications
- Refer to Urinary Tract Infection - Paediatric Empiric Guidelines (ChAMP) for further information.
- Prophylaxis is not routinely used after the first documented UTI.
Oral antibiotic choices for patients ≥ 3 months old who are being discharged from the emergency department (e.g. are systemically well)
Oral cefalexin 20mg/kg/dose (to a maximum of 750mg) 8 hourly2
or
Oral trimethoprim with sulfamethoxazole (co-trimoxazole) 4mg/kg (to a maximum of 160mg trimethoprim component) 12 hourly2
or
Oral Amoxicillin / Clavulanic Acid 25mg/kg/dose (to a maximum 875mg amoxicillin component) 12 hourly3.
The duration of treatment should be:
Intravenous antibiotic choices for children being admitted to hospital
Amoxicillin 50mg/kg 6 hourly (maximum 1g)2
plus Gentamicin
General once daily dosing:
- Children ≥ 1 month old to 10 years old: 7.5mg/kg/dose (to a maximum of 320mg) ONCE daily.
- Children >10 years to 18 years : 6-7mg/kg/dose (to a maximum of 560mg) ONCE daily.
- No further dose increases should be made without consulting infectious diseases, ChAMP or clinical microbiology
Refer to Neonatal Medication Protocols (internal WA Health only) for Neonates
or
Ceftriaxone 50mg/kg once daily (maximum 2g)2 – if penicillin allergy.
Nursing Considerations
- Record a full set of observations on the Observation and Response Chart and with additional information on the Clinical Comments chart. Followed by two hourly temperature, pulse, blood pressure and respirations if clinically unwell.
- Clean catch, midstream or catheter urine sample collection for urine dipstick test + / - sample to be sent for laboratory microculture and sensitivity.
- Analgesia if required.
- Consider topical local anaesthetic e.g. lidocaine (lignocaine) with prilocaine (EMLA®) in preparation for an IV, if clinically unwell or toxic signs are present.
Referrals and follow up
Renal tract ultrasounds
- The following children should have a renal tract ultrasound after discharge from ED
- Less than 3 years old with a first UTI
- Recurrent UTIs
- Atypical organism (e.g. Pseudomonas)
- Not responding to 48 hours of appropriate antibiotics6
GP follow up
- All children presenting with a UTI should have GP follow up within 48-72 hours and a GP letter completed.
- If an ultrasound is indicated and the child’s family has access to reliable GP follow up, advise the GP to arrange and follow up the ultrasound.
Referral to General Paediatric Team
- If an ultrasound is indicated and there are concerns about the family’s ability to access a GP or private radiology, request a PCH outpatient ultrasound and refer to General Paediatrics Outpatient Clinic.
- Children with recurrent UTIs should also be referred even if they have a normal ultrasound.
- Refer to General Paediatric Outpatient Clinic if the renal tract ultrasound is abnormal.
Bibliography
- Bonadio W, Maida G. UTI in outpatient febrile infants younger than 30 days of age: a 10-year evaluation. Pediatr Infect Dis J. 2014;33(4):342
- AMH Children’s Dosing Companion (2022) Australian Medicines Handbook Pty Ltd 2022, Available from: AMH Children's Dosing Companion (health.wa.gov.au)
- Amoxicillin-clavulanic acid Pediatric drug information [Internet]. Lexicomp. [cited 16/06/2022]
- WA Health Child and Adolescent Health Service. Department of General Paediatrics. Urinary Tract Infections: Investigation and Follow Up Clinical Practice Guideline. Version 1: 2015.
- Ismaili K, Lolin K, Damry N, Alexander M, Lepage P, Hall M J. Febrile UTIs in 0- to 3-month-old infants: a prospective follow-up study. Pediatr. 2011;158(1):91.
- Imaging to investigate UTI in children reference: Therapeutic Guidelines eTG [March 2021 Cited: 24 May 2022] Available from: Topic | Therapeutic Guidelines (health.wa.gov.au)
| Endorsed by: |
Drugs and Therapeutics Committee |
Date: |
Jul 2022 |
This document can be made available in alternative formats on request for a person with a disability.